Diagnosing LAM
Because many of the early signs and symptoms of LAM are similar to those of other lung diseases, including asthma, emphysema and bronchitis, LAM can be difficult to diagnose. On average, women with LAM have symptoms for 3 to 5 years and suffer more than two pneumothoraces before the diagnosis of LAM is made.
The most common presentation of LAM is progressive dyspnea on exertion (difficulty breathing with physical activity), often in association with a history of pneumothorax (lung collapse) or chylothorax (collection of lymphatic fluid around the lungs). Pneumothorax can also be the event that suggests the diagnosis of LAM in patients who do not have dyspnea on exertion. Other symptoms of LAM include chest pain or coughing.
High-resolution CT (HRCT) scan is the most accurate imaging test for diagnosing LAM, providing a correct diagnosis more than 80% of the time. HRCT screening for LAM is recommended for all women >18 years with known TSC, women presenting with a spontaneous pneumothorax, and women found to have an angiomyolipoma, abdominal lymphangiomyoma or chylous effusion. The typical HRCT findings of LAM include diffuse, uniform, round, thin-walled cysts, with normal appearing intervening lung parenchyma (Figure 1).

In women with CT findings of cystic lung disease suggestive of LAM, the following stepwise evaluation progressing from least to most invasive means (Figure 2) is recommended to establish a confirmed diagnosis:
- Detailed history and physical examination to evaluate for concomitant tuberous sclerosis complex (TSC). Common skin findings of TSC include: Angiofibromas (acne-like small reddish nodular lesions on the face, especially the nose and cheeks), Subungual fibromas (fibrous nodules arising around or beneath the nails), Shagreen’s patches (rough, elevated lesions commonly seen on the lower back), and Hypomelanotic macular lesions, also referred to as ash leaf lesions (oval or ash leaf-shaped lesions with decreased pigmentation as compared to the surrounding skin).
- Abdominal imaging to evaluate for benign kidney tumors (angiomyolipomas), which are found in 30-40 percent of women with LAM, and can help confirm the diagnosis of LAM.
- Sampling abnormal fluid collections (e.g, chylothorax or ascites) to confirm the presence of chyle.
- Measurement of serum vascular endothelial growth factor-D (VEGF-D) levels can help distinguish LAM from other cystic lung diseases that present with similar HRCT scan appearances. In patients with a compatible HRCT chest, a high VEGF-D value (greater than 800pg/ml) is diagnostic for LAM, and no other confirmatory test is needed in that scenario. Thus, a high VEGF-D level can reduce the need for an invasive lung biopsy to diagnose LAM. It is important to remember, however, that a normal VEGF-D level does not rule out the diagnosis of LAM. High VEGF-D levels are present in ~60% of patients with LAM. VEGF-D levels tend to be higher in LAM patients with lymphatic involvement. Although not fully established, VEGF-D may also be useful as a screening test for LAM in women with TSC. VEGF-D blood tests are assessed at Cincinnati Children’s Hospital Medical Center. For questions about submitting samples in the US and internationally, contact:
https://research.cchmc.org/translationalcores/ttdsl, ttdsl@cchmc.org, 513-636-5998, Procedures for VEGF-D Specimen Collection
UPDATE: VEGF-D TESTING:
VEGF-D testing officially resumed at Cincinnati Children’s the week of February 3rd. Samples are currently being run as FIFO (First In/First Out) with an expected 3-4 week turnaround time. The lab is working as quickly as possible to get through the backlog of samples and hopes to get back to normal turnaround times by the end of March. The website (Cincinnati Children’s Test Directory | Tests) will continue to say the test is offline in the near term, but the lab is working to get the website updated to show availability as well.
The manufacturing issues that caused the testing to stop were confirmed to be resolved by the manufacturer at the start of January, and we don’t anticipate any additional issues at this time.
- The diagnosis of LAM can be established by one of the above means in greater than two-thirds of the patients. In the remaining patients, lung biopsy may be required to obtain a confirmed diagnosis. A transbronchial lung biopsy can be diagnostic in 50-60% of cases of LAM, especially when reviewed by an expert pathologist, and can be the initial mode of acquiring lung tissue. Video-assisted thorascopic surgery (VATS) guided lung biopsy is the gold standard and is diagnostic in virtually every patient.
Additional tests to be considered on a case-by-case basis
- CT or MRI of the head should be considered for cortical tubers or other clinically occult manifestations of TSC.
- Alpha-1 antitrypsin level should be considered to screen for hereditary forms of emphysema.
- Serologies for Sjogren’s disease should be considered, especially if xerostomia (dry mouth) and xeroopthalmia (dry eyes) are present, as Sjogren’s can also present as cystic lung disease that can mimic LAM.
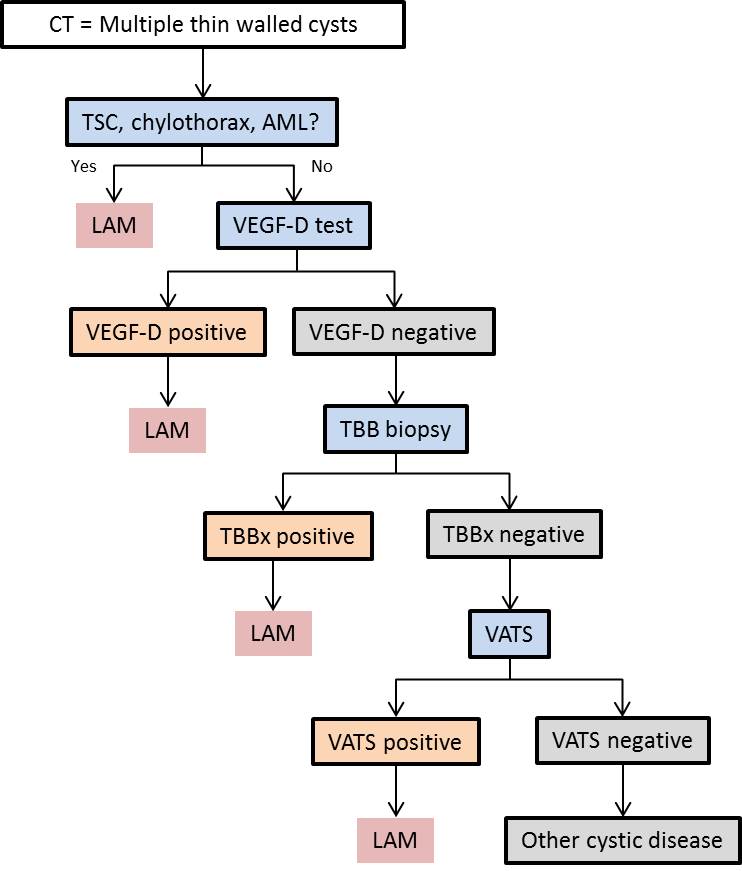
Outlines a proposed algorithm for the diagnosis of LAM. CT: computed tomography; TSC: tuberous sclerosis complex; AML: angiomyolipoma; VEGF-D: vascular endothelial growth factor D; TBBx: transbronchial biopsy; VATS: video-assisted thoracoscopic surgery.
This content was created for general informational purposes only. The content is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.